








Welcome to the Mindset Extended Reality (XR) Innovation Support Programme learning resources, which include three series delivered in conjunction with our expert Mindset-XR programme partners:
• Medical regulation;
• Clinical evidence;
• Lived experience involvement.
Mindset-XR is helping to catalyse the growth of immersive digital mental health solutions in the UK, through funding, tailored support and training. It is delivered by Innovate UK and the Health Innovation Network South London (HIN).
This series focuses on Patient and Public Involvement and Engagement (PPIE), with key insights from MQ Mental Health. Across this module, we provide an accessible introduction to people and companies that want to learn more about patient involvement, with a focus on health technology research. Each module includes additional resources to support your learning and a quiz to test your understanding.
Outline
Welcome to Module 11: Patient and Public Involvement and Engagement (PPIE) in mental health technology research. In this section, we’re focusing on:
What is Patient and Public Involvement and Engagement (PPIE)?
Clarify the concept of PPIE and understand its value in mental health technology research.
The different stages of PPIE
Establishing the key principles and features.
Challenges and best practices
Identifying common challenges in PPIE and strategies to overcome them.
Quiz
Multiple choice questions to test your understanding on Patient and Public Involvement and Engagement.
Watch the video below for an introduction to lived experience involvement.
Glossary
- PPIE – refers to an active partnership between participants and researchers in the research process. Not to be confused with recruitment of participants for studies or product testing. PPIE emphasises the active role of participants in research.
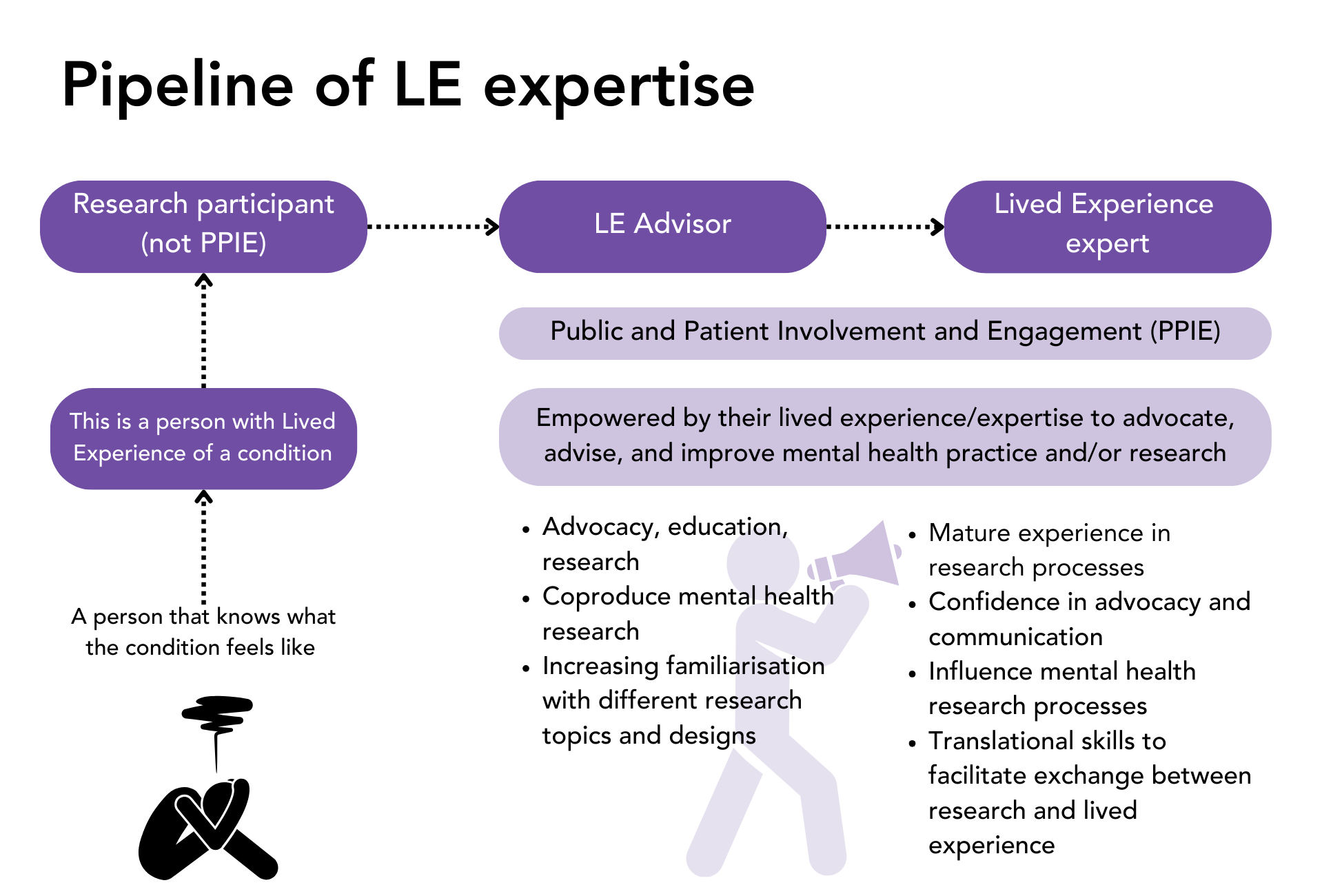
- Lived Experience (LE) – used in this module to describe a person who has knowledge and understanding of a condition due to their first-hand experience of living with it.
- LE expert / LE advisor – individuals who use their lived experience to advocate, advise, and improve mental health practice and/or research.
- Public – in PPIE, this refers to: patients; potential patients, carers; people who use health and social care services; and people from organisations that represent people who use health and social care services.
- Coproduction – the last of four stages of PPIE. It refers to the active involvement of the public in research. This module explores the key principles and features of this stage.
- Psychological safety – a shared belief in a team that members are free to express their ideas, concerns, and questions without fear of negative consequences.
What is Patient and Public Involvement and Engagement (PPIE)?
Officially, the NIHR defines it as follows:
Patient and Public Involvement and Engagement (PPIE), sometimes referred to as “public involvement”, refers to an active partnership between patients, the public, and researchers in the research process. People are not merely ‘subjects’ of research, they are active participants.
- Recruiting participants for a study or product testing is not PPIE – PPIE entails meaningful involvement and influence in the decision-making processes and direction of the research.
Involvement mechanisms can be varied. It is up to the researchers to plan how to involve people in research, identifying which population groups would be best placed to provide valuable insights for the research you are conducting. It requires planning each stage, from the recruitment to how to evaluate and communicate the impact of PPIE activities.
Who is the public?
Various terms are used in the literature and by different organisations to refer to the collaboration between research and people with lived experience of mental health conditions. However, the definitive aspect of PPIE in research is doing research ‘with’ or ‘by’ people who use services rather than ‘to’, ‘about’ or ‘for’ them.
The term “public” in PPIE refers to:
- Patients
- Potential patients
- Carers
- People who use health and social care services
- People from organisations that represent people who use health and social care services
Commonly used terms in PPIE
- Lived Experience (LE)
- People with Lived Experience
- Lived Experience experts
- Experiential advisors
- Public and Patient Involvement and Engagement (PPIE)
- Public and Patient Involvement (PPI)
- Lived Experience involvement and engagement
- Coproduction and lived experience
The importance of PPIE in mental health technology research
Over time, the role of patients and the public in research has therefore evolved from passive subjects to active participants and collaborators, shaping the research agenda, design, and implementation.
Commercial incentives added to a recent explosion of mental health tech products can generate mistrust and make difficult to differentiate those with a solid evidence-based and guided by the aim of improving people’s lives. Sound methods of coproduction with Lived Experience help tech developers to generate trust and buy-in for their products
Involving those with lived experience in research is important to:
- Make products more relevant. Patients and the public have lived experience and detailed knowledge of the issues that matter to them.
- Ensures that research is ethical and accessible.
- Help to accelerate the translation of research into practical applications.
- Help to address digital and mental health inequalities.
- Maximize investment of time and resources.
- Leads to better health and social care services, treatments, and quality of care.
Diversity of lived experience
It is common in the mental health research sector that researchers are themselves people with lived experience of mental health conditions, or practitioners. However, to avoid biases, it is important that there are people exclusively representing the interests and perspectives of people with lived experience.
Through their participation in research PPIE, people with lived experience of mental health conditions develop a specific set of skills. These can be used to improve research and make it more responsive and relevant to the needs and priorities of people affected by a condition. This involvement develops a particular set of capacities that transform a person with lived experience of a mental health condition into a LE expert.
These skills include:
- Understanding of research processes, such as health tech research, pharmacological, psychological, etc.
- Advocacy
- Influencing
- Communication
- Translational capacities (which become more specialised with experience)
- Confidence to raise potential risks
- Question and influence decisions
- Principles of psychological safety should be applied in the PPIE process to encourage Lived Experience experts to express any ideas, concerns, or questions, without fear of negative consequences. The Harvard Business Review piece on psychological safety is a good place to begin to understand and implement the concept.
Background – PPIE in health research
The history of patient and public engagement (PPIE) in UK research has been an iterative process. Despite ongoing challenges, the UK has built a strong foundation for PPIE that continues to evolve to meet the needs of patients, the public, and the research community.
PPIE in UK research began with the patient advocacy movements of the 1960s and 1970s. During this time, there was a growing recognition that patients should have a voice in decisions affecting their health. However, research engagement was limited, with patients seen more as subjects than active participants. 1970s Department of Health – Personal and Public Involvement (PPI) (3).
The 1990s marked a significant turning point with the concept of “public involvement” in research gaining traction. Policy changes and patient group advocacy led to the UK Department of Health’s 1994 “Research for Health” strategy, emphasizing public involvement in health research (4).
In 1996, the establishment of Consumers in NHS Research (later renamed INVOLVE) was a landmark event. INVOLVE supported active public involvement in all stages of research, recognizing the value of experiential knowledge and viewing patients and the public as experts (5). The UK Department of Health published a series of influential documents, including the 1994 “Research for Health” strategy, which emphasised the importance of involving the public in health research.
The early 2000s saw PPIE becoming institutionalized within the UK research landscape. The Research Governance Framework for Health and Social Care (2001) mandated public involvement in research, and funding bodies like the NIHR began requiring PPIE for funding.
The NIHR, established in 2006, played a crucial role in embedding PPI within research practice, promoting it as a key component of high-quality research. It continues to support this role today.
In the 2010s, PPIE grew in prominence and sophistication. The Health Research Authority (HRA), established in 2011, emphasized the ethical imperative of involving patients and the public in research. Guidelines like the UK Standards for Public Involvement in Research (2019) were developed to ensure consistent and meaningful engagement.
There has been a growing recognition of the need to engage diverse and underrepresented groups in research. Initiatives like the NIHR’s INCLUDE project and efforts by the HRA and MHRA aim to ensure research is inclusive and reflective of the broader population (6).
Stages of Patient and Public Involvement and Engagement
PPIE activities entail the recruitment, involvement, and engagement of people with lived experience in research (often called LE advisors or LE experts) up to the stage of coproduction.
Recruitment
The recruitment stage refers to the opportunities to involve people with Lived Experience in research. There are many opportunities throughout the research cycle to involve people although these may differ slightly between research projects.
Recruitment can be conducted through digital and not digital channels depending on the population of interest, as well as on the resources and dissemination channels available to the organisations.
Examples of direct recruitment include:
Social media
Patient groups
Lived Experience networks
Mental health advocacy groups
Involvement
The involvement stage aims to establish an active partnership between patients and the public and researchers in the research process. It entails the establishment of formal governance mechanisms, as well as more informal practices to build trust, rapport, and openness.
Examples include:
Working with research funders to prioritise research
Offering advice as members of a project steering group or advisory board
Developing and giving feedback on research materials
Undertaking interviews with research participants
MindTech is an organisation and national centre focusing on the development, adoption, and evaluation of new technologies for mental healthcare and dementia. They have created this resource – an audiovisual website on how to do good PPI from the Digital youth programme, and featuring many members of MindTech.
Engagement
The engagement stage refers to the different ways in which research can be shared with the public. Engagement encourages researchers to listen and interact with the general public.
For example, researchers may engage with the general public through:
Science festivals
Media coverage
Social media
Multimedia such as blogs, videos, interviews
Dissemination through community workers and organisations
MindTech have produced a series on how to talk to people with lived experience called “What’s up with everyone?“. This resource provides mental health and wellbeing videos developed with Aardman Animations and MindTech.
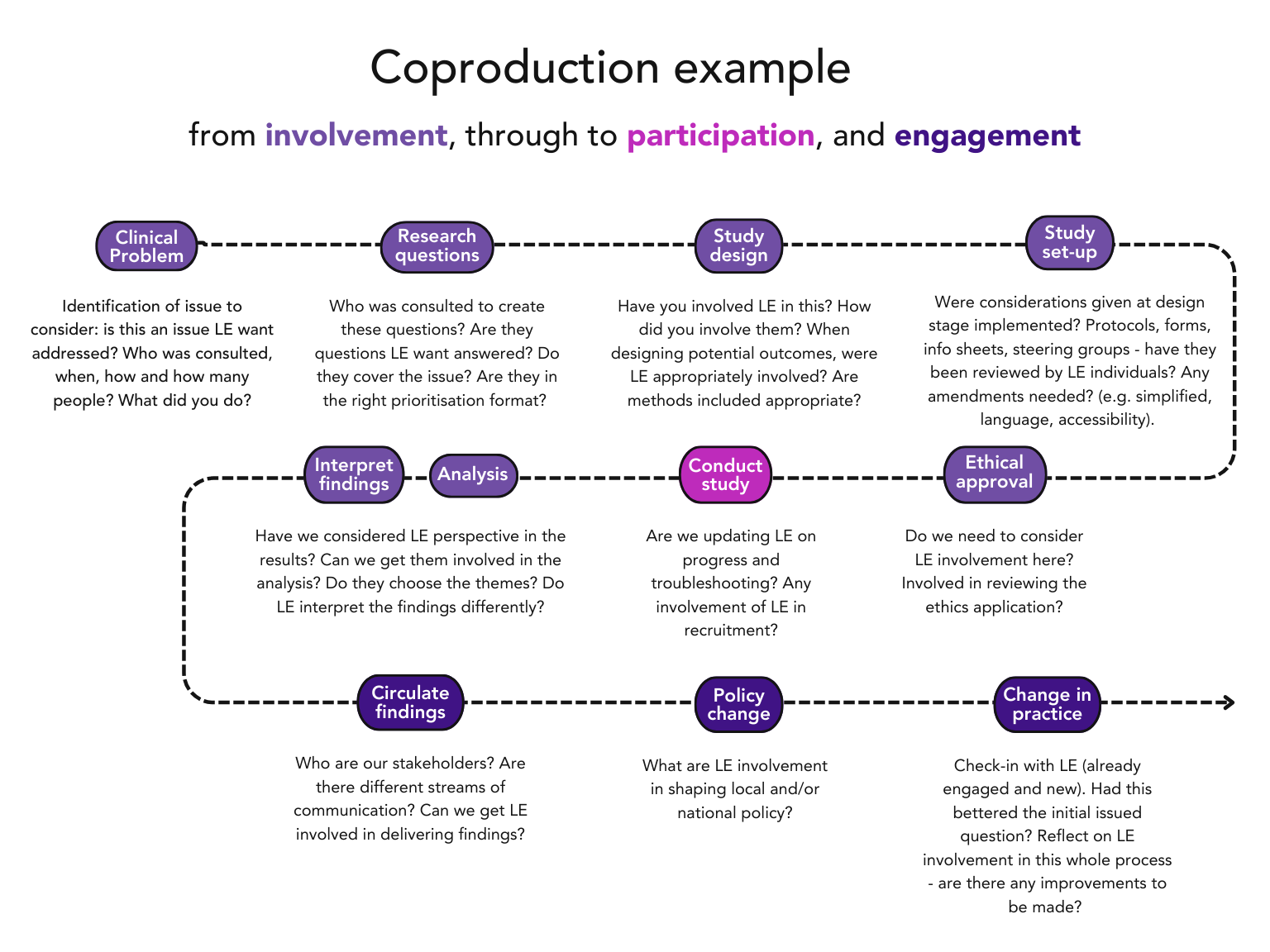
Coproduction
- Coproduction is a term which is increasingly used to refer to involving the public in research.
Co-producing a research project is an approach in which researchers, practitioners and the public work together, sharing power and responsibility from the start to the end of the project, including the generation of knowledge.
It shifts the power and focus on the strengths and expertise of people with lived experience who are involved as co-researchers. Within any co-produced project there must be the acknowledgement that the dynamics and established hierarchies of privileging traditional forms of knowledge and expertise within the research community will not work in co-produced research.
Click the subheadings below to explore the key principles and key features of coproduction.
Key principles
- Sharing of power – the research is jointly owned and people work together to achieve a joint understanding
- Including all perspectives and skills – make sure the research team includes all those who can contribute
- Respecting and valuing the knowledge of all those working together on the research – everyone is of equal importance
- Reciprocity – everybody benefits from working together
- Building and maintaining relationships – an emphasis on relationships is key to sharing power
Key features
- Establishing ground rules
- Continuing dialogue
- Joint ownership of key decisions
- A commitment to relationship building
- Opportunities for personal growth and development
- Flexibility
- Continuous reflection
- Valuing and evaluating the impact of co-producing research
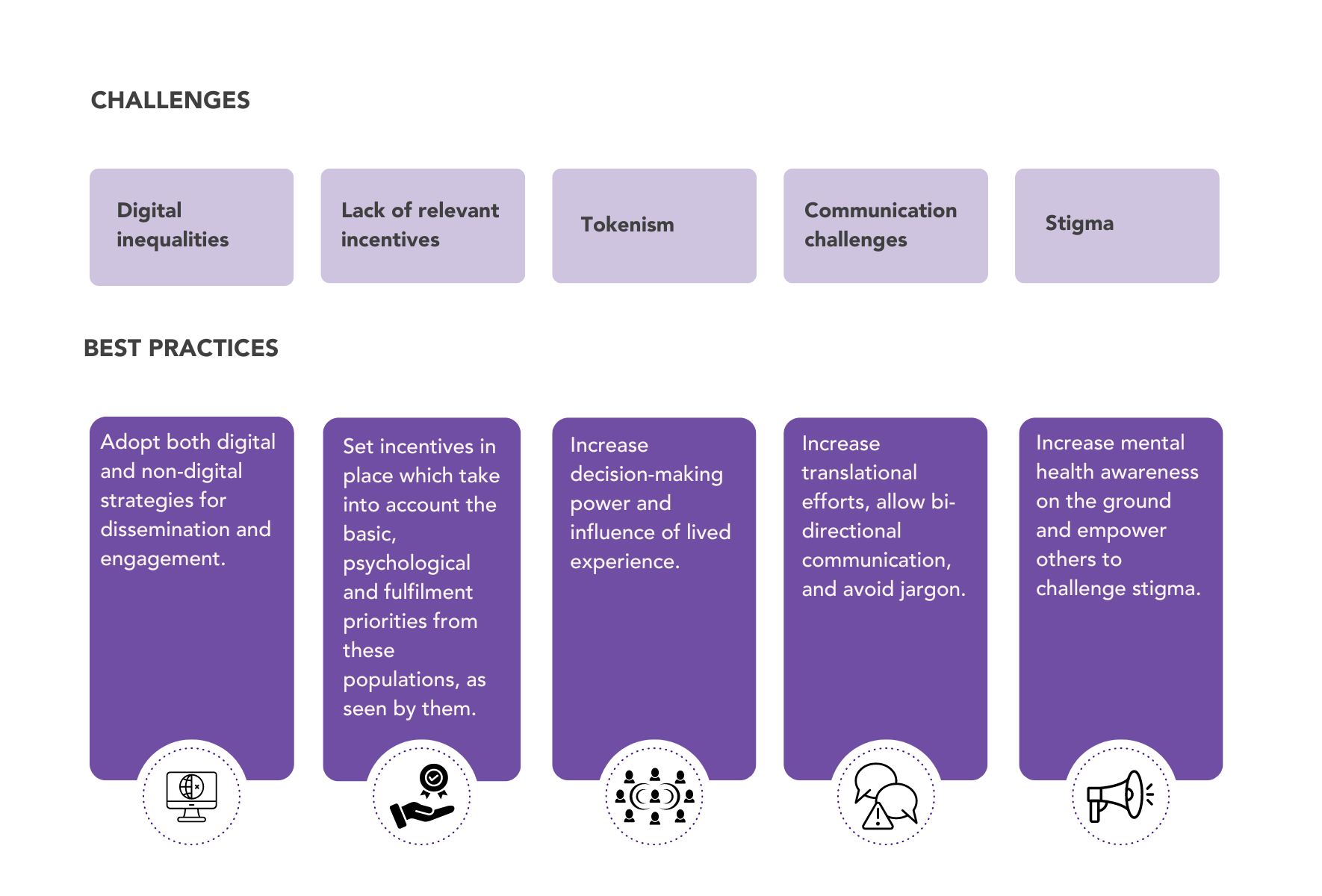
Challenges and best practices in PPIE
Recruitment
Challenges
- Difficulties to reach and inform potential participants about the research being undertaken.
- Lack of relevant incentives for people to participate, considering their needs, priorities and interests.
- Difficulty to reach diversity of Lived Experience participants and people from marginalised and / or under-served communities.
- Identifying individuals with relevant lived experience who also have the interest and ability to contribute to niche fields like virtual and immersive technologies.
Best practices
- Think about innovative ways in which to recruit the people that you want for your project. Most charities have lived experience networks.
- Set appropriate incentives considering the basic, psychological and fulfilment needs of your group of interests. For example:
- Providing monetary or other material compensation
- Promoting career development opportunities through links or mentorships with organisations
- Facilitating participation and covering transportation or internet costs; emphasising the potential impact of the research
- Consider the benefits guideline of NIHR.
- Use both digital and not digital communication channels to reach representatives from underserved and marginalised populations.
- Incorporate standards of Equity, Diversity and Inclusion. There are organisations such as Egality Health who have a range of resources to help widen diversity and inclusion.
- Collaborate with community organizations, advocacy groups, and networks that work with individuals who have relevant lived experiences. These partnerships can help identify potential advisors and build trust.
Involvement
Challenges
- Once advisors are recruited, ensuring their engagement and meaningful participation can be challenging. Advisors may feel their contributions are undervalued or not integrated effectively into the research process.
- Disengagement and a lack of sustained involvement.
- Formal and impersonal research environments can make difficult to build rapport and trust, or for Lived Experience Advisors to share their views openly.
Best practices
- Provide training in lay terms – relevant to what you want them to do.
- Use of glossaries.
- Manage differences and expectations.
- Allow opportunities for informal and unstructured exchanges with the research team, allowing them to humanize themselves, build rapport and trust. This can be through ice-breaking activities or informal debriefs, sharing about hobbies, interests or wider views.
- Be transparent in communications and encourage feedback.
Understand your aims
Ask yourself these questions
- What am I hoping to achieve? / What outcome am I looking for?
- What issue or challenge in my research or research plans could the perspective of the public or experiential knowledge of patient help to overcome?
- What difference or impact do I want this involvement to make?
Engagement
Challenges
- Participating in mental health engagement activities might imply the admission of mental health difficulties to oneself and others, which can be highly stigmatising.
- Research in virtual and immersive technologies often involves technical concepts that can limit the accessibility and comprehension of the research findings, reducing their impact and reach.
- Not everyone has access to the necessary technology to experience virtual and immersive technologies firsthand. This can create a barrier to fully appreciating the research, especially for those who cannot engage with the technology directly.
- Traditional dissemination methods (e.g., academic papers, presentations) may not fully capture the immersive nature of the technology, leading to less impactful dissemination of the research findings.
Best practices
- Consider partnering with community organisations and research charities such as Doctors/Health Centres, Recovery Communities, Shopping Centre billboards and Housing Associations.
- Provide opportunities for Lived Experience Advisors to coauthor publications.
- Ensure that Lived Experience experts who have helped in the research wish to act as advocates, speakers at conferences and events.
- Use simplified language and visual aids (e.g., infographics, videos) to explain complex concepts. Creating engaging and easy-to-understand content can help bridge the gap between technical research and a broader audience.
- Offer accessible demonstrations of the technology, such as online simulations or interactive web-based experiences. Partnering with institutions like museums or educational centers to provide hands-on experiences can also be effective.
Coproduction
Challenges
- Building and maintaining trust and balance of power might be difficult in an environment that is usually researcher led.
- Jargon and technical language might hinder shared understanding.
- Different expectations about the role of Lived Experience Advisors within the research project.
- Tokenism (participation without meaningful influence).
Best practices
- Creating a safe and inclusive environment for all, which must be a priority of engagement and support equality.
- Supporting different ways of partnering, taking time to understand how they feel best placed to contribute and what skills they already have.
- Facilitate an initial dialogue to build shared understanding and expectations about the PPIE practices and the role of Lived Experience Advisors in the project.
- Understand communication preferences among Lived Experience Advisors, including offering plenty of opportunities for meetings and debriefs.
- Adopt a learning by experience approach and encourage open feedback on the PPIE practices.
- Providing training opportunities which requires an ongoing evaluation of needs and tailor-based solutions so that Lived Experience Advisors feel supported.
- Providing glossaries and explaining scientific terms.
- Lived Experience experts should be empowered to influence decisions in research, support translational efforts, and empower others to increase mental health awareness and fight stigma on the ground.
Summary
Patient and Public involvement in research is now regarded as an integral part of any research project.
PPIE entails an active partnership between patients, the public, and researchers in the research process, rather than using people merely as subjects. Researchers plan how to involve people, identify suitable population groups, and evaluate the impact of PPIE activities.
Importance of PPIE in mental health technology research
- Relevance: Makes research more relevant by incorporating lived experiences.
- Ethics and Accessibility: Ensures research is ethical and accessible.
- Practical Applications: Accelerates the translation of research into practical applications.
- Addressing Inequalities: Helps address digital and mental health inequalities.
- Resource Maximization: Maximizes investment of time and resources.
- Improved Services: Leads to better health and social care services, treatments, and quality of care.
Recruitment vs. PPIE
- Recruitment: Involves finding participants for studies.
- PPIE: Entails meaningful involvement and influence in research decision-making processes.
Skills Developed Through PPIE
- Research Understanding: Includes health tech research, pharmacological, psychological, etc.
- Advocacy and Communication: Skills in advocacy, influencing, communication, and translational capacities.
- Confidence and Influence: Confidence to raise potential risks, question, and influence decisions.
Stages of PPIE
- Recruitment: Opportunities to involve people with lived experience in research.
- Involvement: Establishing active partnerships between patients, the public, and researchers.
- Engagement: Sharing research with the public in a two-way process.
- Coproduction: Researchers, practitioners, and the public work together, sharing power and responsibility.
- Principles: Sharing power, including all perspectives, valuing knowledge, reciprocity, building relationships.
Challenges and best practices
Quiz
Resources
MQ Lived Experience Report – click this link to download
MQ Lived Experience Introduction – click this link to download
Additional resources
Digital Youth. (n.d.). Watch & listen. Digital Youth. Retrieved September 5, 2024, from https://digitalyouth.ac.uk/resources/watch-listen/
Cultiv8 Process website: Humanising healthcare – The emergence of experiential practice and leadership in mental health services -Published paper on lived experience practice and models of ‘patient leadership’
Brown, N. J., Lankshear, A., Leroi, I., Bowman, C., Staniszewska, S., Reeves, D., … & Russell, L. (2022). A Journey of Digital Co-Production: Introducing the “E-Nabling Digital Co-Production” Framework and Its Performance in Dementia Research. Research Square. https://doi.org/10.21203/rs.3.rs-2094025/v1
Staniszewska, S., Reeves, D., Leroi, I., Nyman, S. R., Brown, N. J., Ballard, C., … & Lankshear, A. (2022). Insights on conducting digital patient and public involvement in dementia research during the COVID-19 pandemic: supporting the development of an “E-nabling digital co-production” framework. Research Involvement and Engagement, 8, 22. https://doi.org/10.1186/s40900-022-00373-w
Other resources
A Journey of Digital Co-Production: Introducing the “E-Nabling Digital Co-Production” Framework and Its Performance in Dementia Research | Research Square
Patient and Public Involvement (PPI) and Responsible Research and Innovation (RRI) approaches in mental health projects involving young people: a scoping review protocol – PubMed (nih.gov)
Got questions, comments or feedback?Get in touch with the teamhin.mindset@nhs.net

