Blog
Post Title
Claire Torkelson, Diabetes Project Manager at the Health Innovation Network South London, outlines key themes from the Diabetes UK Professional Conference 2026, including unwarranted variation, the shift towards data-driven care, and emerging innovations in type 1 diabetes. She also sets out what these developments mean for the new National Hybrid Closed Loop Adoption and Type 1 Diabetes Outpatient Transformation Programme, delivered in partnership with NHS England to support equitable access to Hybrid Closed Loop technology across England.
On 22 April I had the privilege of representing Health Innovation Network (HIN) South London at the Diabetes UK Professional Conference in Liverpool, joining colleagues from across the field to share learning, hear from researchers, and celebrate the extraordinary moment we find ourselves in for type 1 diabetes care.
The timing felt significant. We have just launched the National Hybrid Closed Loop Adoption and Type 1 Diabetes Outpatient Transformation Programme, which we are delivering alongside NHS England, to support the uptake of Hybrid Closed Loop technology across England.
The conference was a powerful reminder of the ambition and momentum behind this work, and the incredible progress NHS England and our type 1 diabetes services have already achieved only two years into the roll out of this transformative technology.
Addressing unwarranted variation in Hybrid Closed Loop provision
In the opening plenary, NHS England's National Clinical Director for Diabetes and Obesity, Clare Hambling, drew attention to the concept of unwarranted variation, meaning differences in access and outcomes that cannot be explained by patient choice or clinical need. This framing precisely describes the kind of system-driven disparity that our national programme exists to identify and address.
Under NICE Technology Appraisal 943, Hybrid Closed Loop is now recommended for eligible people with type 1 diabetes, a landmark decision that places the NHS at the leading edge of diabetes technology adoption globally. Our role as health innovation networks is to make that recommendation a reality for every eligible patient, regardless of where they live or which service they attend.
As health innovation networks, we can measure variation across ICBs and regions, understand what is driving it, and work alongside clinical services to close the gap. We can bring together teams across England to share intelligence, coordinate delivery, and maintain a consistent focus on equity. National Diabetes Audit data reflects a commitment to equitable roll-out at all system levels, with Hybrid Closed Loop starts distributed more consistently across ethnic and sociodemographic groups. That is a real achievement, and our programme is built to sustain and extend it.
Becoming data-driven: digital enablement, inequalities, and risk stratification
A recurring theme across the conference was the opportunity for services to become data-driven, moving beyond activity reporting to use the information they hold to find patients, understand their populations, and design care around need.
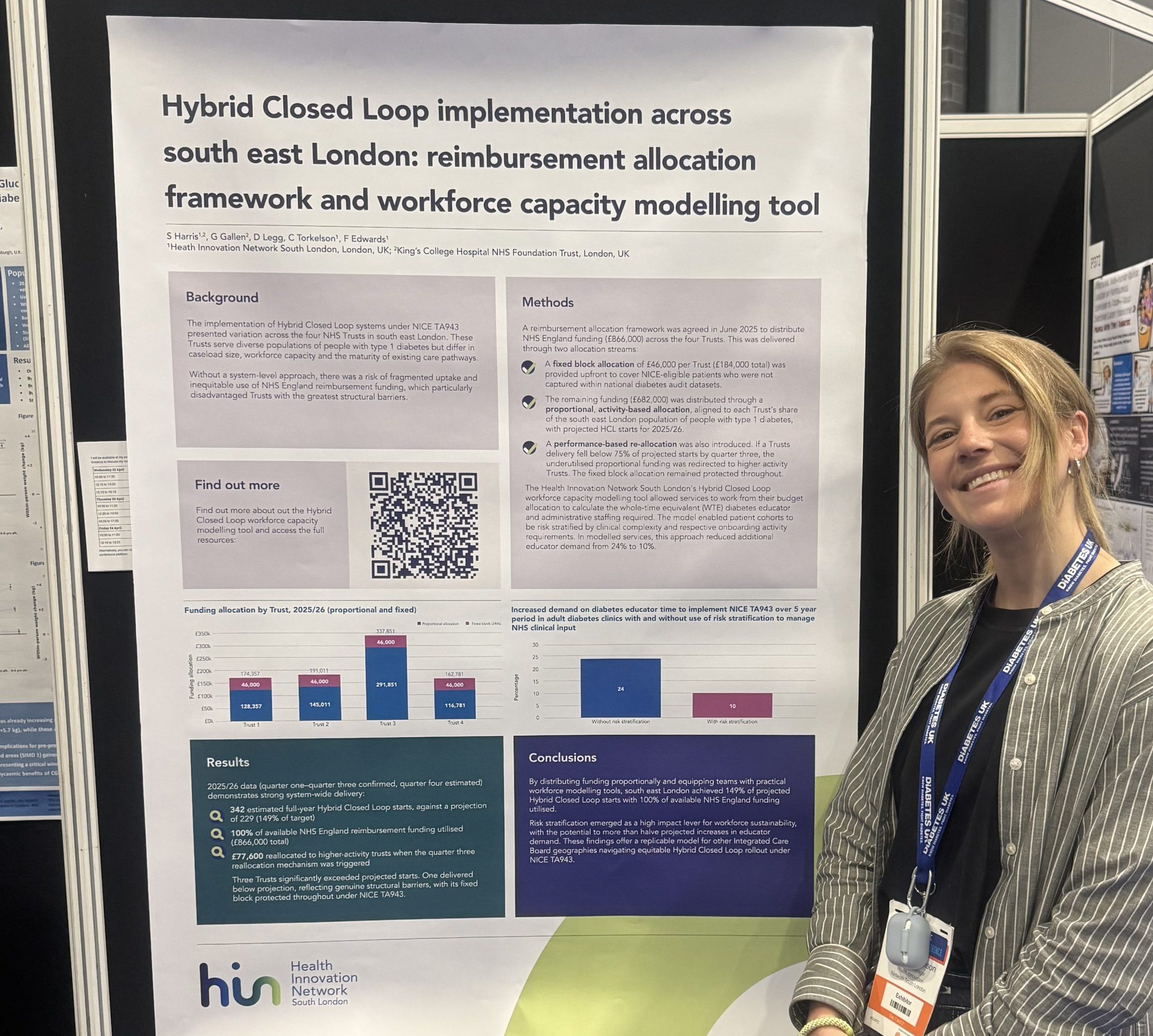
Our programme supports services in building the capability to use that data meaningfully. In 2024-25, we developed and delivered the Hybrid Closed Loop workforce capacity modelling tool, which enables services to plan delivery more effectively by aligning workforce capacity with projected demand. Alongside this, we also provided training resources so care teams can embed regular data review into practice and use risk stratification to proactively identify eligible patients who have not yet been reached.
Planning for the future: screening, innovation, and a new model of care
Some of the most exciting sessions at the conference came from researchers working at the frontier of type 1 diabetes. Representatives from the ELSA and T1DRA screening studies presented compelling evidence for early identification of type 1 diabetes risk. Knowing a diagnosis is likely, before a person becomes dependent on insulin, gives families time to learn, prepare, and engage with clinical teams ahead of time. It reduces the shock of diagnosis, lowers rates of emergency admission, and offers people a far gentler introduction to living with type 1 diabetes.
As well as screenings, faster acting insulin formulations are moving closer to routine availability, and breakthroughs in stem cell therapy are beginning to shift what long-term remission from type 1 diabetes might look like. Technology options are also expanding, with smart multiple-daily-injection therapy emerging as a meaningful step forward for people who are not yet ready for, or suited to, Hybrid Closed Loop, ensuring that the benefits of connected care extend further across the type 1 population.
The second ambition of our programme is to help services position themselves for that future. Hybrid Closed Loop, implemented well, should release clinical capacity, reducing the intensity of routine follow-up for stable patients and freeing teams to focus on complexity, innovation, and the next generation of change. We want to work with services to realise that benefit in practice and to use it as a springboard for embedding new approaches to outpatient care.
Final thoughts
One of the most striking moments of the conference was seeing the trajectory of National Diabetes Audit data over the past decade. The improvements in type 1 diabetes outcomes, including improvements that extend meaningfully across ethnic and sociodemographic lines, are a testament to what sustained, system-wide effort can achieve.
The science is advancing, the policy framework is in place, and the NHS has demonstrated it can deliver equitable, world-leading care in this space. Our national programme is part of that effort, helping to reduce variation, build data-driven services, and prepare the system for the innovations still to come.
It is a genuinely exciting time to be working in type 1 diabetes. If you are involved in delivery and want to find out more about the programme or how your health innovation network can support your ICB, we would love to hear from you.
Get in touch
Find out more about the National Hybrid Closed Loop Adoption and Type 1 Diabetes Outpatient Transformation Programme.
Contact us