Our Mindset-XR Innovation Support Programme spotlight for September is on Sketchbook Games - an indie game studio that promotes wellbeing through emotionally rich, story-driven games that blend art and narrative.
Their flagship title, Lost Words: Beyond the Page, explores themes of loss and healing through a unique blend of journal-based storytelling and platforming.
Below, we hear from founder Mark Backler, who shares insights about the company and its innovative approach to wellbeing.
What three pieces of advice would you give budding innovators?
Solve real problems - Focus on genuine pain points or unmet needs.
Prototype fast, iterate often - Don’t wait for perfection. Build quick, testable versions to learn what works, then refine based on real feedback.
Build a network - Surround yourself with people who challenge, support, and inspire you. Collaboration and mentorship are fuel for innovation.
What is the most exciting statistic or fact you have about XR and mental health?
The use of extended reality (XR) in mental healthcare has been growing rapidly with increasing adoption driven by evidence of its effectiveness in treating conditions like anxiety, PTSD, and phobias.
It’s an exciting time and this momentum is reflected in the growing interest we’ve seen in our own XR solution signalling a strong demand for innovative therapeutic tools.
How has user feedback shaped your product?
User feedback, from academic researchers, users and psychologists, has shaped our XR solution from the start, ensuring it follows therapeutic best practice while remaining safe, engaging, and user-friendly.
These insights have guided the content and exercises to help us ensure they are relevant and meaningful - and this ongoing dialogue continues to make the product more effective and responsive to real-world needs.
What is the biggest challenge you have faced so far in developing your innovation?
Securing funding and sustaining momentum with limited resources has been one of our biggest challenges.
Like many early-stage health tech projects, we’ve had to balance ambition with practicality in pushing development, testing, and iteration without long-term financial security.
As a small team, we are strategic in focus and often multitask across roles.
These constraints ultimately make us lean, focused, and adaptable, which are qualities that strengthen our innovation.
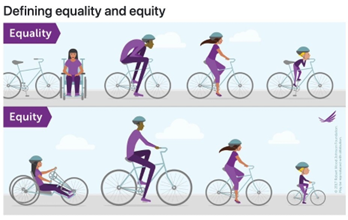
How could your innovation tackle inequalities in mental health?
Our games make mental health support more accessible, relatable, and engaging. XR delivers therapeutic content in a flexible, scalable format that reaches beyond clinical settings, including remote or underserved communities with limited access to in-person services.
It also reduces stigma by offering a private, self-paced way to engage with support, which is especially valuable where seeking help is taboo. In this way, our innovation can bridge gaps in access, representation, and experience, helping to reduce inequalities in mental healthcare delivery and outcomes.
Why should the health and care system be excited about your innovation?
Our games are highly engaging so they can help with ensuring patients remain active and involved in their care and treatment.
Our innovation offers a preventative and engaging tool that complements traditional mental health support.
What XR success stories would you like to share with us?
We'd like to share a BBC News report called Industry welcomes first wave of pensioner gamers plus a report on BBC Look East about the sector with an interview with founder Mark Backler (2:27) and footage of Soul Garden (3:21).
What type of support are you seeking most from readers to help drive your project forward?
We’re primarily seeking partnerships and funding to help scale our impact. Specifically:
1. Connections to mental health organisations for collaboration and research validation.
2. Funding or investment to expand development and reach more users.
3. Opportunities to pilot within health or educational settings to test and refine the experience.
Get in touch at info@scenegraphstudios.com. We'd love to hear from you.
Want to find out more about our Mindset-XR Innovation Support Programme?
Sign up to our monthly newsletter and keep up to date with all the latest news
Click here